The dusty binders may be gone. Walk into most hospitals today, and you’ll find fewer filing cabinets stuffed with outdated policies. Instead, the graveyard has moved online.
Today’s “document graveyard” is SharePoint sites, intranet folders, and static PDF repositories. Policies technically exist in digital form, but for frontline staff, they might as well be buried six feet under. Clunky navigation, siloed folders, and poor search functionality mean that critical documents are effectively invisible when they’re needed most.
The risks are no less real than in the paper era. They may be greater. When leaders believe they’ve modernised simply because documents are “online,” they risk overlooking the ways these legacy digital systems fail to protect staff, patients, and the organisation itself.
Clinical Risk: When ‘Online’ Isn’t Accessible
In healthcare settings, SharePoint and intranet-based repositories were an important first step in moving away from paper-based policy management. But they were never designed for the complex demands of modern healthcare. These systems are effective at storing documents, yet storage alone isn’t enough when staff and regulators need instant access, clear version control, and evidence of staff attestation.
The result?
❌ Staff waste valuable time scrolling through endless lists of documents.
❌ Different teams create duplicate versions, leading to confusion about which is correct.
❌ Staff rely on memory, peer advice, or outdated hard copies because they can’t reliably find what they need.
Clinical risk doesn’t just come from the absence of policies. It also comes from policies that staff can’t quickly find, trust, or use.
““Healthcare can’t afford to treat policy management as an administrative afterthought. Outdated or inaccessible documents don’t just create inefficiency, they put patients, staff, and organisations at real risk.””
Compliance Risk: Regulators Aren’t Fooled
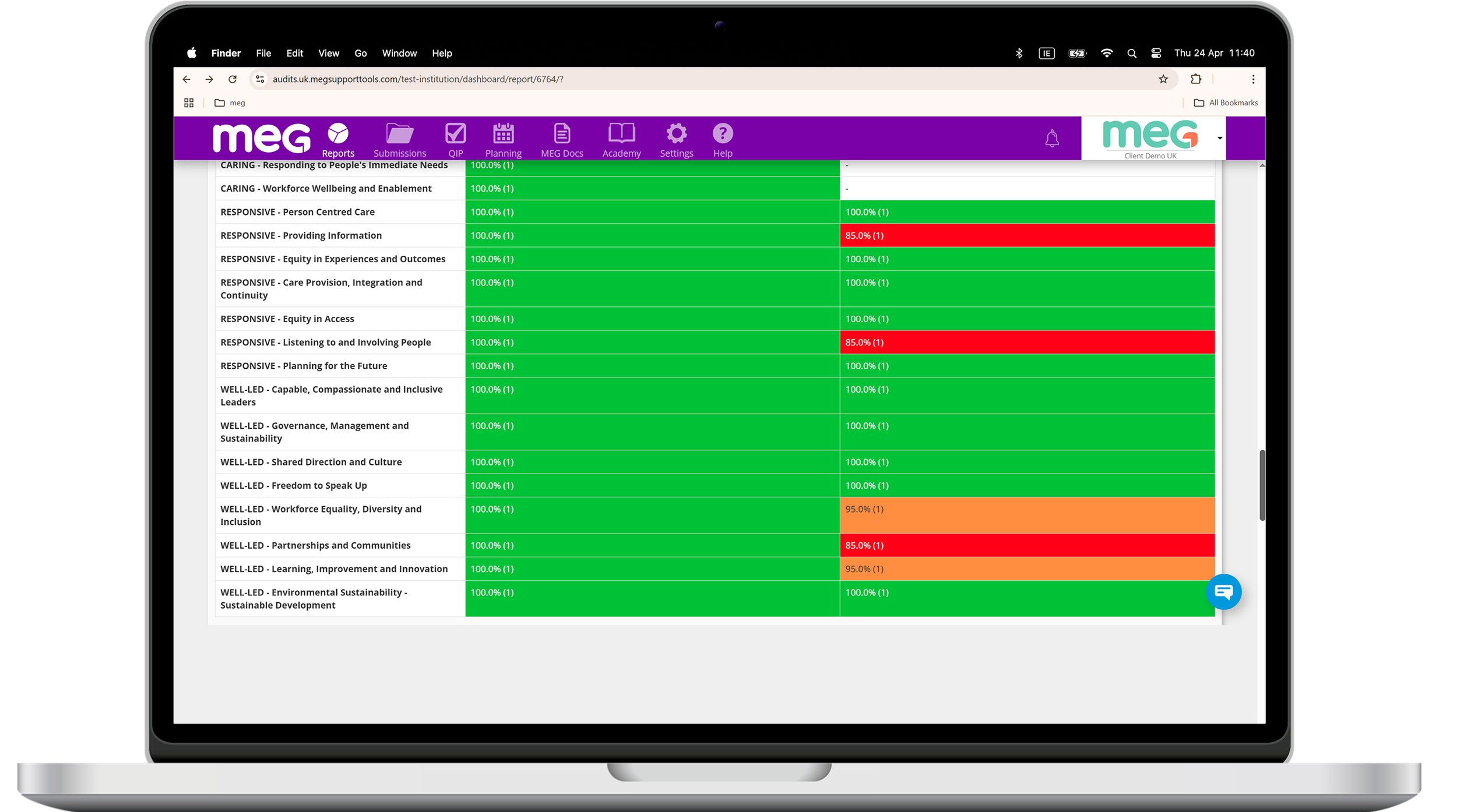
Healthcare regulators expect more than “documents stored somewhere online.” All require clear version control, audit trails, and demonstrable accessibility as a minimum standard.
Legacy systems often fall short:
Multiple versions of the same policy may live in different folders.
No reliable audit trail shows who reviewed or approved changes.
Surveyors asking “show me the policy” are met with frantic searches and uncertain results.
Most critically: attestation is nearly impossible.
SharePoint and intranets can’t track whether staff have actually opened, read, and acknowledged a policy.
There’s no way to assign policies to specific roles and capture individual attestations.
Leaders are left hoping staff are compliant — but with no evidence to prove it when regulators ask.
In compliance terms, “we emailed it” or “it’s in SharePoint” doesn’t demonstrate accountability. Regulators want to see that staff received, read, and signed off on policies — and that organizations can prove it with a clear audit trail.
Cultural Risk: The Cost of Mistrust
Culture is built on trust. Staff need to believe that leadership equips them with the tools and information to succeed.
When staff can’t reliably find policies, frustration grows. Over time, disengagement sets in. They create workarounds, pass around shadow documents, or simply rely on “what we’ve always done.”
This doesn’t just weaken compliance; it corrodes culture. Staff begin to assume leadership doesn’t prioritise their needs. That mistrust spreads, undermining safety culture and reducing adherence to policies across the board.
A graveyard system doesn’t just bury documents. It buries staff morale.
The Illusion of Modernisation
The danger of legacy digital systems is that they create a false sense of progress. Leaders may think, “We’ve digitised our policies, so we’re fine.”
But digitisation is not the same as accessibility. Putting binders online doesn’t solve the problem; it only relocates it.
If a nurse spends 10 minutes searching for the infection control policy…
If a compliance officer can’t instantly demonstrate the current version to an inspector or accreditation surveyor…
If a new junior doctor downloads an outdated PDF from a shared drive…
…then the system isn’t modern. It’s a digital graveyard, and the risks are very much alive.
Why This Matters Now
Healthcare is under more pressure than ever:
Staffing shortages mean new hires must be onboarded quickly and reliably.
Regulatory scrutiny is increasing, with zero tolerance for “we couldn’t find it.”
Patient safety demands require information that is trusted, consistent, and easy to locate in the moment of need.
Legacy digital systems were an important step away from paper, but they simply weren’t built for this environment. What’s needed is not just digitisation, but transformation: systems designed for findability, trust, and accountability.
Retiring the Digital Graveyard
It’s time to face reality: SharePoint and other intranet repositories were built for document storage, not for the complex demands of healthcare policy management. They remain useful as general collaboration tools, but they can’t provide the speed, visibility, and proof that today’s healthcare environment requires.
Healthcare leaders must demand more:
Powerful search that delivers the right policy in seconds.
Real-time version control that eliminates duplicates and confusion.
Audit trails and reporting that satisfy regulators.
Attestation tools that prove staff have read and understood critical policies.
The graveyard metaphor still applies but the solution is clear. Policies must be living documents, searchable in seconds, validated by audit trails, and supported by staff attestations.
Conclusion
The binders may be gone, but the graveyard remains. It lives in outdated digital systems that are siloed, clunky, and difficult to search with confidence.
Legacy systems multiply clinical, compliance, and cultural risks. And in a healthcare environment where every second counts, that’s unacceptable.
Healthcare leaders must move beyond the illusion of digitisation. Retiring the digital graveyard means adopting policy management systems that are dynamic, searchable, and accountable.
Because when policies are buried, whether in basements, in outdated PDFs, or in SharePoint with no proof they’ve been read, risk comes to life.
👉 In Part 2, we’ll explore how MEG transforms document management from a passive repository into a living, connected quality engine, giving healthcare leaders the tools to reduce risk, improve compliance, and empower staff with information they can trust.
Watch the On-Demand Webinar
Want to explore practical steps for moving beyond the “digital graveyard”? Watch our on-demand webinar:
“Is Your Document System Driving Improvement, Or Just Storing Policies?”
🎙 Featuring Clare Harney, Head of Advisory & Education Services at Santegic, and Leonora O’Brien, Chief Growth Officer at MEG